Traditional spine surgery, involving the treatment of degenerative conditions of the spine- herniated discs, spinal stenosis and spondylolisthesis (spinal misalignment) - requires larger skin incisions, with the dissection of the surrounding ligaments and stripping of the paraspinous musculature. This process can often result in damage to the ligaments and musculature of the spine by affecting the underlying neural and blood supply. Injury to these supporting structures can often weaken them and also produce persistent postoperative pain.
Traditional spine surgery, involving the treatment of degenerative conditions of the spine- herniated discs, spinal stenosis and spondylolisthesis (spinal misalignment) - requires larger skin incisions, with the dissection of the surrounding ligaments and stripping of the paraspinous musculature. This process can often result in damage to the ligaments and musculature of the spine by affecting the underlying neural and blood supply. Injury to these supporting structures can often weaken them and also produce persistent postoperative pain.
Technological advancements in equipment and instrumentation such as digital fluoroscopy, image guidance, high-resolution endoscopy and microscopy along with tubular dilators and working channels have allowed for the development of minimally invasive surgical (MIS) techniques for the surgical treatment of degenerative spinal disorders. The fundamental philosophy of MIS procedures is to minimize approach-related morbidity. Utilizing small portals of entry or working corridors, injury to the surrounding muscles and ligaments of the spine is minimized. Once appropriate access is obtained, the same surgical objectives of decompression of the neural elements and/or stabilization of the spine may be accomplished. Therefore, perhaps the term “minimal access” is a more accurate description.
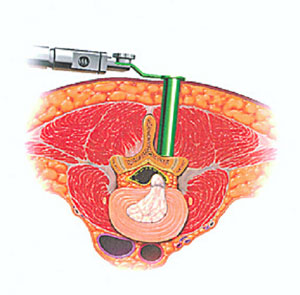
To summarize, the concept of minimal access spine surgery involves the use of dilators to split the fibers of the paraspinous musculature. This muscle splitting approach markedly reduces injury to the muscles and also limits dissection of the ligaments. A tubular-type retractor is then placed over the dilators and docked on the spine. (Figures 1 & 2) Utilizing magnification provided by an endoscope or microscope, based upon surgeon preference, decompression of the neural elements may be carried out and if necessary, grafts placed for fusion. Instrumentation may then be placed either through expandable tubes or directly through very small skin incisions.
Figure 1 – Standard subperiosteal muscle dissection
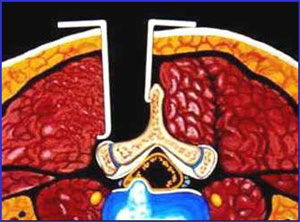
Figure 2 – Muscle splitting, minimal access approach